
HIV is quite important in the world of medicine, so here is my list of ‘things to know about HIV’ and a checklist of points, to help med students remember the key aspects of the disease.
If you think of something that should be included, fire away and I’ll add it!
Definition and Criteria
What is HIV?
- Human Immunodeficiency Virus
- HIV-1
- M (main) – 90% of infection worldwide
- 9 subtypes or clades
- A-D – Americas and Western Europe are mainly clade B
- F-H – Much more variation in Asia and Africa
- J
- K
- and many recombinant forms
- 9 subtypes or clades
- N (new)
- O (outlier)
- M (main) – 90% of infection worldwide
- HIV-2 (less common)
- HIV-1
- A retrovirus identified in the eighties
- The virus binds the CD4 cell at the CD4 receptor and at a coreceptor
- CXCR4 or
- CCR5
What is seroconversion?
- a period of time, when HIV antibodies develop and start to be detectable in the blood
- takes place within a few weeks of infection
- usually accompanied by seroconversion illness or acute retroviral syndrome:
- fever
- rash
- muscle aches and joint pain
- lymphadenopathy
- less common:
- headaches
- diarrhoea
- sore throat
- What is important about seroconversion illness?
- usually resolves in 2-3 weeks
- SUPREMELY infectious during this point
- very unreliable as a way of diagnosing HIV as so non-specific
How is it transmitted?
- Found in bodily fluids
- Transmission through
- anal, vaginal and oral sexual contact
- sharing needles
- mother to baby (vertical transmission) through pregnancy, birth or breastfeeding
What’s an opportunistic infection?
- An infection that takes advantage of the fact that the immune system is compromised to flourish.
- AIDS-defining conditions:
- Pneumocystis pneumonia (name carinii is sometimes replaced by jiroveci)
- Diagnosis
- Investigations
- Management
- Medications
- Prevention
- Diagnosis
- Toxoplasma encephalitis
- Kaposi’s sarcoma
- Cryptococcal meningitis
- Mycobacterium tuberculosis
- Lymphoma
- Cryptosporidosis
- CMV (not in liver, spleen or nodes)
- Oesophageal candidiasis
- Recurrent pneumonia
- Progressive Multifocal Leukoencephalopathy
- Chronic herpes simplex ulcers
- Salmonella septicaemia
- Pneumocystis pneumonia (name carinii is sometimes replaced by jiroveci)
Epidemiology
- At the end of 2014 there were 103,700 people living with HIV in the UK
- 43,000 MSM
- 1/20 MSM are HIV positive
- 54,000 Heterosexual men and women
- 1/56 Black African men
- 1/22 Black African women
- 17% of those with the condition do not know they are infected
- 43,000 MSM
History
- Discovered in the 80s when 5 MSM were diagnosed with Pneumocystis Carnii Pneumonia
- only really affects severely immunocompromised
- Incurable, no treatment, terminal
- Management largely palliative
- Huge stigma attached to diagnosis due to
- sexual transmission
- association with drug users
Diagnosis
What’s a window period?
- The time in which the markers of infection are not yet detectable
- after infection, before seroconversion
- about a month for HIV
- testing before this leads to false negatives
- don’t discourage testing in this time, but ensure they’re retested later (12 weeks)
- a 4th generation lab test for HIV after 4 weeks is highly likely to be accurate
- Usually an ELISA
- Positive results are confirmed with a Western Blot
- this is more specific and helps reduce false positives
- Positive results are confirmed with a Western Blot
- Usually an ELISA
What are the CDC criteria for HIV?
- Based on the lowest recorded CD4 count (ever recorded for that patient)
- CD4 count puts you in your number group:
- >500 = 1
- 200-499 = 2
- <200 = 3
- Clinical group puts you in your letter group:
- Asymptomatic/Acute HIV/PGL (persistent generalised lymphadenopathy) = A
- Symptomatic = B
- AIDS-defining condition = C
- Overall results:
- If you are A3, B3 or any of C1-3, you are considered to have AIDS
- CD4 count puts you in your number group:
What are the WHO clinical stages for HIV/AIDS in adults and adolescents?
- Primary HIV
- asymptomatic
- acute retroviral syndrome
- Clinical stage 1
- asymptomatic
- persistent generalised lymphadenopathy
- Clinical stage 2
- moderate unexplained weight loss (<10% of body weight)
- recurrent respiratory infection
- HZV
- angular cheilitis
- recurrent oral ulceration
- papular pruritic eruptions
- seborrhoeic dermatitis
- fungal nail infections
- Clinical stage 3
- severe unexplained weight loss (>10%)
- unexplained diarrhoea >1 month
- oral hairy leukoplakia
- persistent oral candidiasis
- persistent unexplained fever >1 month
- pulmonary TB
- neutropenia/anaemia/thrombocytopenia
- severe bacterial infections
- Clinical stage 4
- AIDS-defining illness
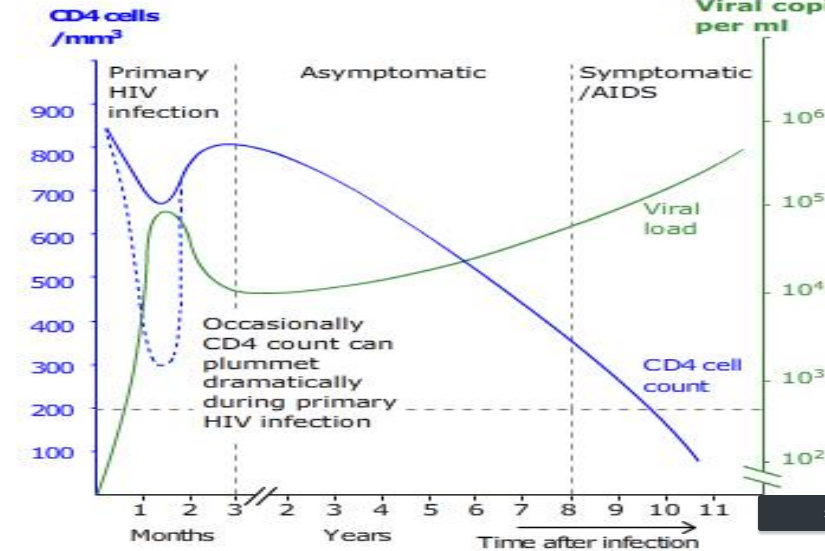
Evolution
If left untreated, HIV tends to follow a fairly predictable pathway from intial infection to AIDS.
- Primary infection
- until seroconversion, when the body and virus reach a state of ‘equilibrium’, which is known as chronic infection
- Chronic infection
- This varies in length, but averages around 10 years
- Infection, cell turnover, viral production and destruction are all very much active during this period of ‘stalemate’
- Most sufferers will see a gradual decline in CD4 levels and immune function
- usually 50-90 cells/microlitre/year
- this rate accelerates as time goes on
Host factors affecting rate of evolution:
- older age
- more rapid disease progression with shorter survival
- Co receptor genotype
- some fortunate individuals have a mutation (delta-32) of the CCR5 co-receptor, which essentially confers almost complete immunity to infection by HIV
- These all accelerate the course of disease:
- unprotected anal intercourse
- smoking
- depression
Complications
What are the consequences of late presentation?
- Increased rate of opportunistic infection
- Increased recurrence of OI
- Increased rate of AIDS and death
- In general, late presentation is declining in the West, due to screening programmes and better diagnosis
What are the clinical manifestations of advanced disease?
- Rash
- Shortness of breath/cough
- Loss of consciousness/Hemiparesis
- Meningism/Headache
- Decline in cognition
- Visual disturbance
- Diarrhoea
- Wasting
- Jaundice
What are the indications for caring for an HIV infected person in isolation on a ward?
- In general HIV patients do not need isolation as they’re not going to give the virus to anyone else
- If however they have respiratory symptoms, or diarrhoea and vomiting, they should be isolated as any other patient would
- special precaution should be taken as the infection is more likely to be ‘atypical’ than in an ‘ordinary’ D+V or RTI patient
- If however they have respiratory symptoms, or diarrhoea and vomiting, they should be isolated as any other patient would
What are the commonest tumours in HIV?
- The following are AIDS-defining
- Kaposi sarcoma
- Non-Hodgkin lymphoma
- Cervical cancer
- Other common ones
- anal
- liver
- lung
- Hodgkin
What are the commonest mycobacterial infections in HIV?
- Mycobacterium tuberculosis
- Mycobacterium avium
- Mycobacterium intracellulare
- Mycobacterium kansasaii
- Mycobacterium haemophilum
- understandably these are quite tricky to differentiate between and can all cause quite similar presentations
What are the common fungi in HIV?
- Cryptococcus
- Candidiasis
- Histoplasmosis
- Sporothrix Schenckii
- Dermatophytes
- What are the associated drugs that are used?
- Nystatin
- Fluconazole
- note that these often suppress, rather than eliminate the infection, as host immunity is required together with anti-fungals to totally eradicate the mycosis
Prognosis
How long can you live with HIV?
- Research in 2008 suggests most people will die with HIV not of HIV
- Many will be able to live well into their seventies
What factors affect prognosis in HIV?
- CD4 count – gives idea of state of immune system (rough idea)
- Viral load – amount of HIV in the blood
- Age
- Comorbidities
- especially Hepatitis B/C
- cardiovascular disease
- liver disease
- cancers
- comorbities have been shown to accelerate progression of HIV, even when controlled for CD4 level
- IVDU
Management and Treatment
What are the principles of HIV treatment?
- The medications available are designed to stop the infection of the immune cells and reduce the amount of virus in the body
- Fusion and entry inhibitors
- Maraviroc
- T-20
- Reverse transcriptase inhibitors
- to prevent production of viral DNA
- Nucleotide Reverse Transcriptase Inhibitors (NRTI)
- Atripla
- Combivir
- Kivexa
- Trizivir
- Truvada
- 3TC
- Abacavir
- Tenofovir
- FTC
- AZT
- ddI
- d4T
- Non-Nucleotide (NNRTI)
- Efavirenz
- Etravirine
- Nevaripine
- Nucleotide Reverse Transcriptase Inhibitors (NRTI)
- to prevent production of viral DNA
- Integrase inhibitors
- to prevent incorporation of viral DNA into the host genome
- Raltegravir
- to prevent incorporation of viral DNA into the host genome
- Protease inhibitors
- to prevent production of new virions
- Atazanavir
- Darunavir
- Fosamprenavir
- Indinavir
- Ritonavir
- Nelfinavir
- Ritonavir
- Saquinavir
- Tipranavir
- to prevent production of new virions
- Fusion and entry inhibitors
- A combination of drugs is used, as the virus can mutate rapidly enough to become resistant to one drug during the treatment
- Fixed dose combinations are where two or more drugs have been combined in a single pill to reduce the pill load for the patient and improve compliance
When should you treat?
- It might seem obvious that one would always treat straight away, however the CDC recommends that if a patient has sufficiently high CD4 count, low viral load and no clinical manifestations, then treatment should not be commenced until one of these indicators suggests to:
- Patient may suffer side effects from the treatment
- Patient may not be psychologically ready to deal with the illness and the medication, and non-compliance or partial-adherence are very dangerous as they facilitate rapid development of resistance to medication
- Patient may have other psychosocial barriers to effective treatment
- Use the interim period to educate the patient, establish a firm support network and ensure that when the time to begin treatment comes, they are ready to use it to its full potential
- the key is to monitor these patients very closely!
- Definitely treat if:
- If positive for Hepatitis B or C, treat when CD4 <500
- If the patient is on radiotherapy or chemotherapy
- If positive for tuberculosis
- HIV-related nephropathy
- HIV-related neurocognitive decline
- CD4 count <200 (ideally start at 350)
How can you monitor the disease?
- Before commencing treatment, monthly blood tests to monitor the effect on the immune system:
- CD4 count
- measuring the percentage of T cells that are CD4 positive, or the CD4/CD8 ratio is a good idea, as it gives a clearer idea as to whether a drop/rise in CD4 is due to a drop in white cells overall (eg infection), or whether it is CD4-specific
- after treatment begins, CD4 count starts to rise (if successful)
- The first rise (1-3 months) is though to be due to redistribution of CD4 cells trapped in lymphoid tissue
- after treatment begins, CD4 count starts to rise (if successful)
- measuring the percentage of T cells that are CD4 positive, or the CD4/CD8 ratio is a good idea, as it gives a clearer idea as to whether a drop/rise in CD4 is due to a drop in white cells overall (eg infection), or whether it is CD4-specific
- Viral load
- the main indicator of successful therapy – a decline in viral load demonstrates the treatment is working
- rule of thumb – decline of 1 log viral load in 4 weeks = success
- decline is usually biphasic
- phase 1 – within first two weeks
- possibly the direct effect of the medications
- phase 2 – later on
- probably the immune system has got back on its feet and can start fighting properly
- phase 1 – within first two weeks
- the main indicator of successful therapy – a decline in viral load demonstrates the treatment is working
- CD4 count
A cool analogy – The Train Model (thanks to John Coffin of Tufts University, around 1996)
Imagine the patient is a train, hurtling towards an impending obstacle, representing an opportunistic infection or onset of AIDS. The CD4 count tells you the distance of the train from the obstacle, while the viral load tells you the speed of the train.
What’s Immune Reconstitution Syndrome?
- As treatment begins to work, the immune system experiences the same thing as a gym rat on a triple dose of pre-workout, and starts to go berserk
- Any opportunistic infection will appear to flare up, as a vigorous inflammatory response is mounted
- Particularly in those with low CD4 counts
- Generally affects the tissues where the infection is concentrated:
- lymphadenopathy in TB
- potentially sight-threatening vitreous inflammation in CMV retinitis
Why might treatment fail?
- Poor adherence to treatment regime
- Unacceptable side effects
- Poor absorption/bioavailability
- Interactions with other drugs
- Drug resistance
How to change regime?
- Try to change one drug at a time
- Ensure none of the other factors are causing an issue
- Keep the patient’s desires and best interests in mind
What are the interactions between medications that can occur?
- The two drugs most likely to interact with recreational drugs are:
- ritonavir
- cobicistat
- these interact with:
- Cystal meth
- MDMA
- Mephedrone
- Ketamine
- Viagra
- Benzodiazepines
- these interact with:
What is PEPSE?
- Post-exposure prophylaxis following sexual exposure
- Emergency prophylaxis can be effective up to 72 hours after exposure, however it should be commenced as soon as possible
- Once the virus reaches the regional lymph nodes it replicates very rapidly, and becomes an irreversible infection
- PEP is a month-long course of medication, which can cause side effects and isn’t guaranteed to work
- When to prescribe it
What is primary prophylaxis?
- Preventing opportunistic infections with medication
What is secondary prophylaxis?
- Preventing recurrence of opportunistic infections
What other healthcare requirements are there for people with HIV?
- Huge psychological implications (see below)
- All patients should be screened for:
- Hepatitis:
- A
- B
- C
- and immunised or treated where appropriate
- Syphilis
- Gonorrhoea
- Chlamydia
- Tuberculosis
- Hepatitis:
- Annual vaccination
- pneumococcal
- influenza
- note that vaccines only really work if CD4 >200 so maybe wait until then
What should I super-not do?
- Do not give live vaccines to HIV patients or their contacts
- Oral Polio
- Smallpox
- MMR should be weighed up pros vs cons
Psychological effects
There is a complex two-way relationship between HIV and the psychological health of the patient:
- HIV can predispose to:
- anxiety
- depression
- substance abuse
- Mental illness can:
- reduce compliance with medication
- increase rate of decline
- increase chance of opportunistic infection
Risk factors for transmission
- Sexuality
- Men that have sex with men (MSM)
- Location
- High HIV prevalence
- Recipients of blood transfusion products before 1984
- Risky behaviour
- Alcohol
- Drugs
- multiple sexual partners
- work in sex industry
- Sexual health
- A concurrent STI can increase risk of transmission of HIV
- The presence of genital ulcers
- A high viral load increases the chance of transmission greatly
- conversely a very low count almost eradicates the possibility of transmission
- eg if left untreated, 25% of HIV positive mothers will pass their infection onto their child
- With prenatal antiretroviral therapy, this almost reaches 0%
- eg if left untreated, 25% of HIV positive mothers will pass their infection onto their child
- conversely a very low count almost eradicates the possibility of transmission
- A concurrent STI can increase risk of transmission of HIV
HIV cannot be transmitted through:
- coughing/sneezing
- kissing
- shaking hands
- mosquito/animal bites
- using the same toilet
Prevention:
- Condoms are 69% effective against HIV transmission
The HIV Test
Where can people get a test?
- GUM clinic
- some charities (Terence Higgins Trust)
- antenatal clinic if pregnant
- GP surgery
- some sexual health clinics
- home testing kits
Pre-test discussion:
- Inform person as to why they might choose to have a test done
- Assess risk factors for HIV
- Prepare for a positive diagnosis
- What do you expect the result to show?
- If it is positive, what will you do to deal with the situation?
- What support networks does the person have?
- Do they know what the next steps are if positive (medical and emotional support)
- Build rapport
- Obtain consent for the test
- Must be competent
- Must understand the following features of the test:
- it’s purpose
- benefits
- if positive – access to therapy and support
- if negative – further risk reduction
- knowing HIV status
- protect sexual partners
- reduce transmission
- harms
- psychological impact
- stigma and confidentiality issues
- effect on relationships
- implications for insurance/employment
- risks associated with not being tested
- understand difference between HIV/AIDS
- Must volunteer their consent, not be coerced
- Health promotion
- Safer sex
- advice about sharing needles
- condom use
- screen for other infections
- contraception
- Partner notification
- Does a family member/friend/partner know you’re testing?
- Who would you tell about the result?
- Who would need to know?
- Do they have to tell? GP/Dentist/Schools
- Closure
- Would they like to go ahead?
- Document written/verbal consent
- When will the information be available?
- How will it be available?
- Is referral appropriate
Why people might request a test?
- Personal or partner’s sexual risk
- IVDU
- Pre-op assessment
- Physical symptoms
- Partner or previous partner was HIV +
- Routine antenatal test
- New relationship
- STI screen
- Worried well
- Assault/rape victim
- Blood donation
- Pre/post exposure prophylaxis
- Post needle stick
- Pre-employment
- Life insurance
- New drug therapies
Giving a positive test result:
- be clear and concise
- do not apologise
- let the patient guide the consultation
- focus on what they’re going to do next
- check who knows the client is testing
- respect the client’s views and opinions
- possible arrangements for a confirmatory test
- liaise with HIV team if on the ward
- refer as appropriate
References:
http://www.aidsmap.com/hiv-basics/HIV-AIDS/page/1412437/
http://aidsetc.org/printpdf/9246
http://www.nhs.uk/conditions/HIV/Pages/Introduction.aspx
http://hivinsite.ucsf.edu/InSite?page=kb-03-01-01#S4X
http://www.ncbi.nlm.nih.gov/pubmed/17926639
http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1001510
http://www.uptodate.com/contents/symptoms-of-hiv-infection-beyond-the-basics
https://www.mc.vanderbilt.edu/root/vumc.php?site=infectioncontrol&doc=12978
http://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hiv-fact-sheet
